OneTemplate Coding [TM00042]
Purpose:
This template is for use by clinical coders when receiving external communications from other agencies.
What does it actually do?
It is designed to contain everything a clinical coding team would need to process letters, record relevant information for QOF and ensure that all information received from third parties is recorded accurately and with consistent coding.
This includes:
General information
- Recording the type of communication received
- Recording a 111 disposition
- Recording a cancelled/rearranged/DNA appointment
- Recording admissions and discharges
Observations
This page allows for the recording of important social information - such as smoking or alcohol intake, as well as common examinations such as height, weight, BMI and blood pressure
Actions
This page allows for the recording of specific actions that may be required in primary care, such as:
- suture removal
- blood test
- GP review
- medication request
- onward referral
Allergies and adverse reactions
This page allows the user to record any allergies or adverse reactions
Cancer
This page allows for specific information to be recorded about patients with a cancer diagnosis - recording:
- Chemotherapy
- Radiotherapy
- Hormone therapy
- Brachytherapy
It also gives users supporting information they may wish to send to the patient as well as allowing the recording of gold standards framework status
Screening
On this page, users can record screening information about:
- Cervical screening
- Breast screening
- Bowel cancer screening
- Abdominal aortic aneurysm screening
- Retinal screening
Procedures
This page allows for the recording of common procedures undertaken in secondary care settings, such as:
- Biopsy
- Appendicectomy
- Cholecystectomy
- Tonsillectomy
- Colonoscopy
- Cystoscopy
- Colposcopy
- Duodenoscopy
- Endoscopy
- Gastroscopy
- Laparoscopy
- Sigmoidoscopy
Common scores
Users can record common scoring metrics here:
- QScores, such as QRISK3 and QDiabetes
- PHQ9 or GAD7
- Addenbrooke's Cognitive Examination score and GP COG
Results
This page allows for the standardised recording of results -
For blood results:
- FBCs, U&Es, LFTs
- Prostate Specific Antigen
- Lipids including total cholesterol, HDL, nHDL, LDL and Chol/HDL ratio alongside triglycerides
- Thyroid Function Test including T3 and T4
- HbA1c
Cardiology results:
- Echocardiogram
- Electrocardiogram (ECG)
- Ambulatory ECG
Radiology results:
- Xray
- CT scan
- MRI scan
- Ultrasound scan
- DEXA scan
Fracture
This page allows users to record fractures and flags for consideration of fragility fractures.
QOF & IIF
This page allows users to record key information for QOF and IIF indicators.
For new diagnoses it will show codes relating to tests or referrals that are required, please note these sections will show for all patients regardless of any existing diagnosis. It allows for this information to be recorded in a straightforward way to minimise the need for correcting of coding later on.
The page will also show areas of QOF where the patient already has a diagnosis. These sections will show data needed for specific areas relevant to the patient, so that if any of the data needed is recorded in the communication then this can be added to the record easily, using the correct codes.
What does it look like?
The following are a couple of examples of the pages, and how they appear: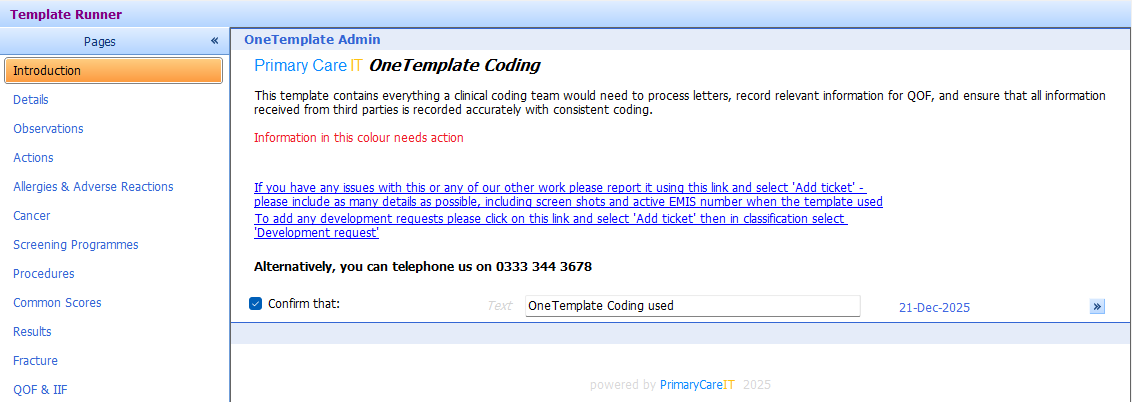
System Dependencies:
There are no dependencies for this template.
Fitting your practice
There aren't any alterations needed to your practice to utilise this template. Your clinical coders need to know that it exists and how to find it.
How to get it
This template will be automatically installed in your system and can be accessed via locating the template, or via the OneLaunchers.
Support Information
Communications Log
Published 15/11/2022.
Primary Care IT are pleased to announce the release of our new OneTemplate coding. This template contains everything that a clinical coding team would need to be effective in their work. It aids teams to record information in a structured and consistent way. Where new diagnoses have required contractual actions, these are highlighted. Where common procedures have been performed in secondary care or where follow up in primary care is needed, users can record this in a standardised way using the template. Where a patient has QOF or IIF actions needed, these are highlighted to the coders, so that if any relevant data is contained within the communication this can be added to the record. We will be rolling this out to all subscribers over the coming weeks. If you are waiting for installation and want us to prioritise your site please submit a ticket to request this.
Related Articles
OneTemplate Admin
Purpose: This template is designed for use by admin team members to record all of the common things that are needed in that role. If there are things that as an admin team member you are regularly doing and want this building into the template, ...OneTemplate Additional Roles
Overview This template has been created for the following purposes: to be used by your additional roles team members to record activity and information to be used for patients to aid with personalised care planning and proactive care. The OneTemplate ...OneTemplate NonPrescriber
Introduction This is a dynamic template for managing chronic disease - so only things that are relevant to the patient you have in front of you are displayed. For example, if the patient is diabetic the diabetes section will show; if they aren't it ...OneTemplate Prescriber
This is a dynamic template for managing chronic disease - so only things that are relevant to the patient you have in front of you are displayed. For example, if the patient is diabetic the diabetes section will show; if they aren't it won't. It’s ...OneTemplate Acute
Introduction This template aids data entry for the commonest consultation types in Primary Care. It can be especially useful for trainees, allied health professionals or even established GPs who just want a structured and evidence based way of ...