Overview
This template has been created for the following purposes:
- to be used by your additional roles team members to record activity and information
- to be used for patients to aid with personalised care planning and proactive care.

The OneTemplate Additional Roles can be opened using the OneLauncher Additional Roles. If you would like further information about this please see our
OneLauncher Additional Roles support article.
The template is based on the specification for the Additional Roles Reimbursement Scheme (ARRS) and it supports the clinician/user in following key clinical, technical and administrative responsibilities in delivering health services.
There are different pages on the template for all of the different Additional Roles Reimbursement Scheme team members, as well as pages which cover all elements required for care planning including:
- Recording important social information needed for a CGA/care planning:
- People involved in the patients care
- Carer details
- Social information
- Managing Care Homes - both intial assessment of new patients and ward round activity
- ARRS team resources
- All pharmacist related activity
- Undertaking Structured Medication reviews
- Undertaking reconcilliation of medication
- Managing DOAC prescribing and monitoring
- Managing anticholinergic burden assessment
- Social prescriber related activity
- Mental health worker related activity
- Dietician related activity
- First contact Physiotherapist related activity
- Managing falls risk and frailty
- Creating a comprehensive Geriatric Assessment (CGA)
- Creating a Personalised Care and Support Plan
How is the template supposed to work in practice?
The idea with this template is that all Additional Roles Team members can use it and input information into the template which can then contribute to the creation of a CGA/Personalised Care and Support Plan. So for example, a pharmacist can undertake a structured medication review, but also use the "People involved" page to record information about others involved with the patients care. A social prescriber may then see the same patient and update information on the "Social information" page. The GP can then review the information entered by the two other team members and complete the "Care Planning" page, then creating the Personalised Care and Support Plan which pulls in all information entered by these three professionals into the singular document.

Users should dip into and dip out of each of the relevant pages as they need, completing elements that they have covered during a consultation. No one user could ever complete all elements of the template in a single consultation.

The "Everything" Page includes all elements required to undertake a CGA and Personalised Care and Support plan in one place - and can be used to easily enter all the information in one place.
What pages does the template contain?
- Introduction
- Everything
- Common Tools
- Quick-Referral to ARRS
- Falls/Frailty
- Care Homes
- People Involved
- Carer Details
- Social Information
- Social Prescriber
- Mental Health
- Dietician
- Pharm Review
- Pharm Reconcilliation
- DOACs
- ACB Medication
- Physiotherapy
- CGA
- Care Planning
In the detail below, we will cover each page of the template. The headings identify the pages of the template, and the lower level headings identify each section within the template.
Introduction Page
This page of the template contains some general information about the template, some information about the person seeing the patient, a section to record proactive care, another to record consent/shared decision making and then there are two sections that will flag if the patient being reviewed has an eFI which suggests moderate or severe frailty. These are covered in more detail below:
About this template
This section introduces the template and provides visual color guidance for navigating different elements. It includes direct links to the support team, enabling quick troubleshooting or the submission of development requests. Users also find the office contact number, and automatically-generated details confirm when the template was used.
Seen by
This area allows users to document who performed the patient consultation, including the presence of a chaperone or interpreter. Having this information readily accessible improves record accuracy and ensures clear communication between healthcare providers.
Living in a care home? (for PCN DES)
Proactive Care
Here, users can record whether proactive care is being offered. These codes are extracted for monitoring purposes related to the PCN DES, although they are not used for payment. The section’s streamlined design ensures quick and efficient data entry for clinicians during consultations.
Consent/Shared decision making
In this section, clinicians can document patient consent to share their health information within the broader care team. This feature is especially useful when multiple healthcare professionals, potentially from different organizations, are involved in the patient's care. Documenting consent upfront can prevent delays and ensure smooth communication across teams.
eFI calculates moderate or severe frailty
This prompt appears if the patient's automatically generated frailty index (eFI) suggests moderate or severe frailty. The tool reminds clinicians to complete a thorough frailty assessment and provides links to resources for managing frail patients. It also includes options for recording consent for additional Summary Care Record (SCR) data sets and noting specific details, such as door code consent.
Everything Page
This page is a comprehensive tool designed to display all relevant patient information in one location. It consolidates data from every page in the template, making it invaluable for care planning. Due to the amount of data included, this page may take a few seconds to load, but the convenience of having all information in one place significantly reduces the need for navigation across multiple pages.
The Everything Page is particularly useful during Multidisciplinary Team (MDT) meetings, where having a complete overview of the patient’s health and care history is crucial. By allowing the entire care team to access and update the patient’s record in real-time, the page promotes cohesive care planning and minimizes potential gaps in communication between different team members.
While this page serves as an all-encompassing hub for care planning, individual sections of the template are covered in greater detail in the support document. It is recommended to use the Everything Page when a broad overview is needed but to navigate through specific pages when detailed entries are required.
Common Tools Page
This page contains some common tools that are likely to be used by Additional Roles team members. For a wider selection of clinical calculators we would suggest use of the
OneCalculator template.
PHQ-9
This can be used to screen patients for depression:
GAD7
This can be used to screen patients for anxiety:
eFI
This can be used to calculate the patients eFI. This score gives an indication of frailty. Frailty is however a clinical diagnosis and clinical correlation using a tool such as the Rockwood Score is recommended.
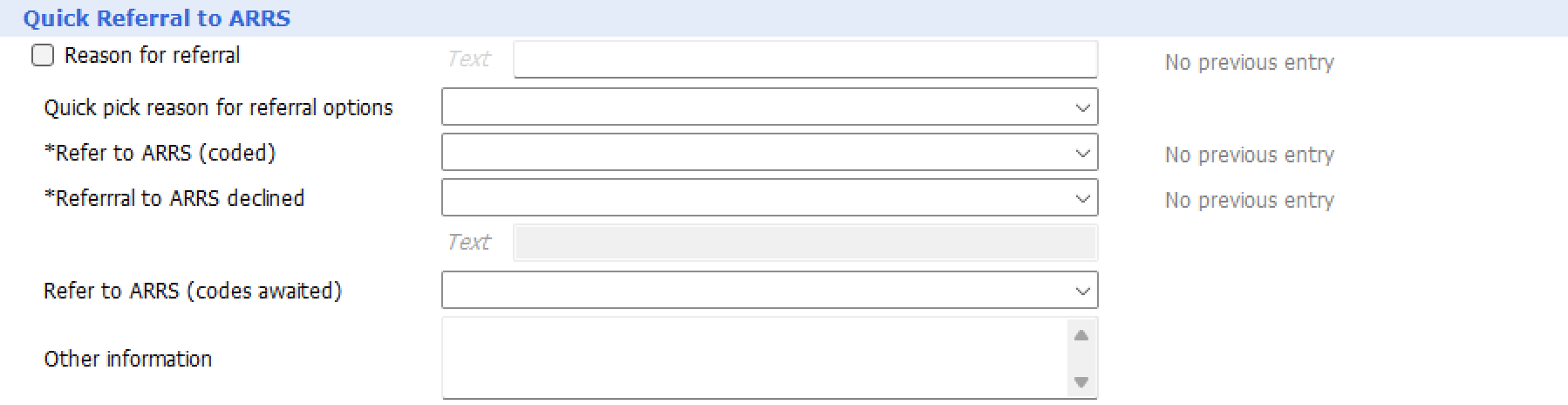
Quick-Referral Page
The Quick-Referral Page simplifies the process of referring patients to Additional Roles Reimbursement Scheme (ARRS) team members. This section is designed for efficient documentation and helps standardize referral information across practices, ensuring consistency in data collection and reporting. This standardized approach allows practices and Primary Care Networks (PCNs) to track activity and demonstrate the impact of ARRS team members within the healthcare system.
Key Elements:
Referral Reason:
This section allows the user to document the specific reason for the referral, providing a clear understanding of the patient’s needs and helping the receiving clinician prioritize care.
ARRS Team Member Selection:
Users can specify which ARRS team member (e.g., Clinical Pharmacist, Social Prescriber, Mental Health Worker, etc.) the patient is being referred to. This clarity ensures the correct healthcare professional is assigned to address the patient’s condition or concern.
Standardized Reporting:
By using consistent coding and documentation, the Quick-Referral Page ensures that referral data can be easily extracted and reported. This reporting is crucial for monitoring the activity and effectiveness of ARRS team members, which is a key aspect of PCN funding and service evaluation.
The Quick-Referral Page is a vital part of the template that encourages a smooth referral process and supports collaborative working across the wider healthcare team. It ensures patients are quickly and effectively referred to the right professionals, enhancing the overall efficiency of care delivery.
Falls/Frailty Page
The Falls/Frailty Page is an essential part of the template, designed to guide clinicians through a thorough assessment of a patient's risk for falls and frailty. Falls are a major concern for elderly or vulnerable patients, and this page offers prompts and tools that assist healthcare professionals in identifying and documenting key risk factors.
Guidance
This section provides a link to the latest NICE Guidance on Falls Assessment, ensuring that clinicians are following evidence-based best practices. Clinicians can refer to this guidance as needed during consultations to ensure they are considering all appropriate factors in the assessment.
Frailty assessment
This section allows users to record a frailty diagnosis. A link to the Rockwood Clinical Frailty Scale is included, giving clinicians a quick reference to the descriptors for each score on the scale. This ensures consistency in frailty assessments across different team members. Clinicians can document the assessment results and note any interventions or referrals needed.
eFI
This tool calculates the patient's frailty index. While the eFI gives a good indication of frailty, clinical correlation is important. It’s recommended that clinicians use the Rockwood Score or another clinical tool alongside the eFI to ensure a comprehensive frailty assessment.
FRAT stands for "Falls Risk Assessment Tool". The FRAT is a validated score used to assess a patient's risk of falls. This section guides the clinician through completing the assessment, covering the main factors associated with increased fall risk. Understanding a patient's fall risk enables clinicians to take proactive steps in reducing this risk, whether through interventions or referrals to other team members.
Falls Assessment
Here, users can record details of any falls the patient has experienced, including the number of falls and a narrative about each incident. Clinicians are encouraged to document their assessment of the likely cause of the falls, which could range from muscle weakness to environmental hazards.
Gait, balance and mobility, and muscle weakness
This section prompts clinicians to assess the patient’s gait, balance, mobility, and muscle strength, which are key indicators of fall risk. Detailed information can be further recorded on the Social Information page if necessary, to build a fuller picture of the patient’s physical abilities.
Osteoporosis Assessment
Clinicians can assess and document the patient's risk for osteoporosis, which increases the risk of fractures in the event of a fall. Guidance is provided to help clinicians identify patients at risk and ensure appropriate management strategies are put in place.
Perceived impaired functional ability and fear relating to falling
This section addresses a common issue where patients with a fear of falling are often more likely to experience a fall. Clinicians are prompted to assess whether this fear is present and how it impacts the patient's daily activities.
Visual impairment
Visual impairment can significantly increase the risk of falls. This section reminds clinicians to screen for any vision problems, with the option to record more detailed information in the Social Information page.
Cognitive, neurological and cardiovascular problems
Many falls are linked to underlying cognitive, neurological, or cardiovascular issues. This section prompts the clinician to consider and document any conditions that may be contributing to the patient’s fall risk.
Continence
Urinary or bowel incontinence can increase a patient’s fall risk, as they may rush to the bathroom, leading to unsteadiness. This section allows users to record whether continence is a concern for the patient.
Home Hazards
Patients who have hazards in their home environment are at a higher risk of falls. Clinicians should enquire about the home environment, though an in-home assessment may be the most accurate way to identify these risks.
Polypharmacy
Patients on multiple medications (polypharmacy) are at greater risk of falls, especially if certain medications contribute to dizziness or confusion. This section flags patients with polypharmacy and encourages a referral to a pharmacist or prescriber for a Structured Medication Review to evaluate the appropriateness of their medication regimen.
Care Homes Page
The Care Homes Page is specifically designed to support healthcare professionals managing patients in care or nursing homes. It helps ensure that all necessary information is captured and recorded consistently during care home visits, whether for initial assessments, ward rounds, or follow-up reviews.
New Resident
This section allows clinicians to quickly document when a patient is newly admitted to a care home. While there are no formal targets for coding care home residency, it is an important metric that is often reviewed by NHS England. Correctly coding patients as residing in care homes ensures accurate reporting and helps practices meet contractual requirements.
Purpose of visit
Clinicians can select the type of visit they are conducting, such as an initial assessment or a follow-up visit. For regular care home patients, this section simplifies the process of recording weekly ward round activity or post-discharge reviews. The clear labeling of visit types ensures accurate and concise documentation.
PCN DES codes
This section consolidates relevant SNOMED codes required for the Primary Care Network Directed Enhanced Service (PCN DES). These codes are extracted from clinical systems and used to monitor activity related to the Enhanced Health in Care Homes (EHCH) scheme. Having these codes accessible during consultations allows clinicians to record the required information without navigating through multiple sections of the patient record.
Ward Round Review: History
During weekly ward rounds, clinicians can record a concise history of the patient's condition, helping to track progress over time. This section is designed to capture changes in the patient’s health status and allows for an ongoing narrative to build across multiple visits.
Ward Round Review: Examination
For patients requiring physical examinations during the ward round, this section enables clinicians to document examination findings consistently. Having this information readily available ensures all team members have a clear picture of the patient’s health.
Mental Capacity
This section supports documentation related to the assessment of a patient’s mental capacity. Clinicians can record whether a formal mental capacity assessment was conducted and note any referrals made to social services or the involvement of an Independent Mental Capacity Advocate (IMCA). This is critical when decisions regarding the patient's care or future planning need to be made.
Preferences for future care
Many patients in care homes are approaching the later stages of life, and discussions about preferences for future care are common. This section allows clinicians to document any conversations around preferred places of care or death, which can be revisited and updated as necessary.
Deprivation of liberty
If a patient has been deprived of their liberty, this section provides space to record details of the DoLS application and outcome. Proper documentation ensures that all team members are aware of any restrictions placed on the patient’s freedom and that appropriate legal safeguards are followed.
The Care Homes Page ensures that all relevant aspects of care are documented thoroughly, enhancing the continuity of care for patients living in care homes and supporting the multidisciplinary team in delivering proactive, patient-centered care.
People Involved Page
The People Involved Page is a crucial tool for documenting and maintaining an up-to-date list of healthcare professionals and others involved in a patient's care. As patients often receive care from multiple team members, particularly in complex cases involving Additional Roles staff, this page helps ensure that everyone involved is visible to all team members, promoting cohesive and collaborative care.
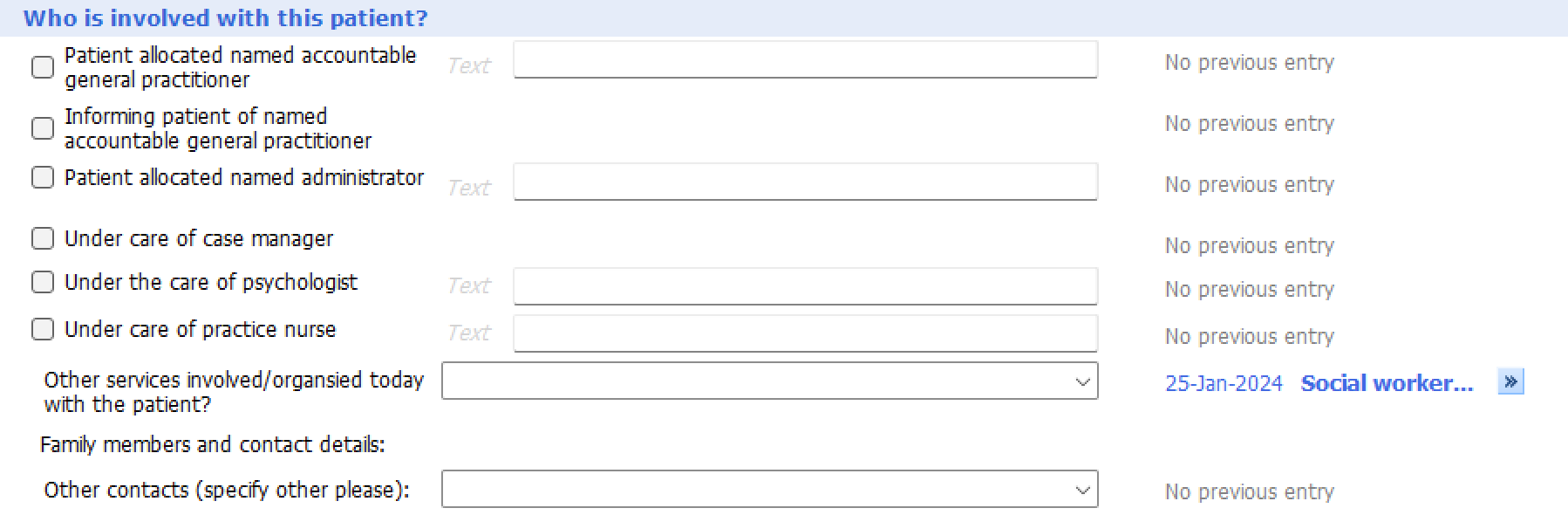
Who is involved with this patient?
This section allows users to quickly record the details of all individuals currently involved in the patient’s care. This is particularly useful when the patient has multiple caregivers or is supported by an interdisciplinary team that spans different services (e.g., GPs, pharmacists, social prescribers, mental health workers, etc.).
Accurate and clear documentation of the care team helps avoid duplication of efforts and ensures that each team member understands the broader care plan for the patient. It also provides quick visibility to other team members, reducing the chance of missed communication between professionals.
Clinicians can update this page as the care team changes over time, ensuring the patient’s record reflects the most current and accurate information. This is especially helpful when multiple professionals are involved, as it enables better coordination and ensures that everyone is aligned with the patient’s needs and ongoing care plans.
The People Involved Page is a central communication hub, enabling an integrated care approach where all relevant team members are easily identified and where collaboration is fostered through clear visibility of roles.
Carer Details Page
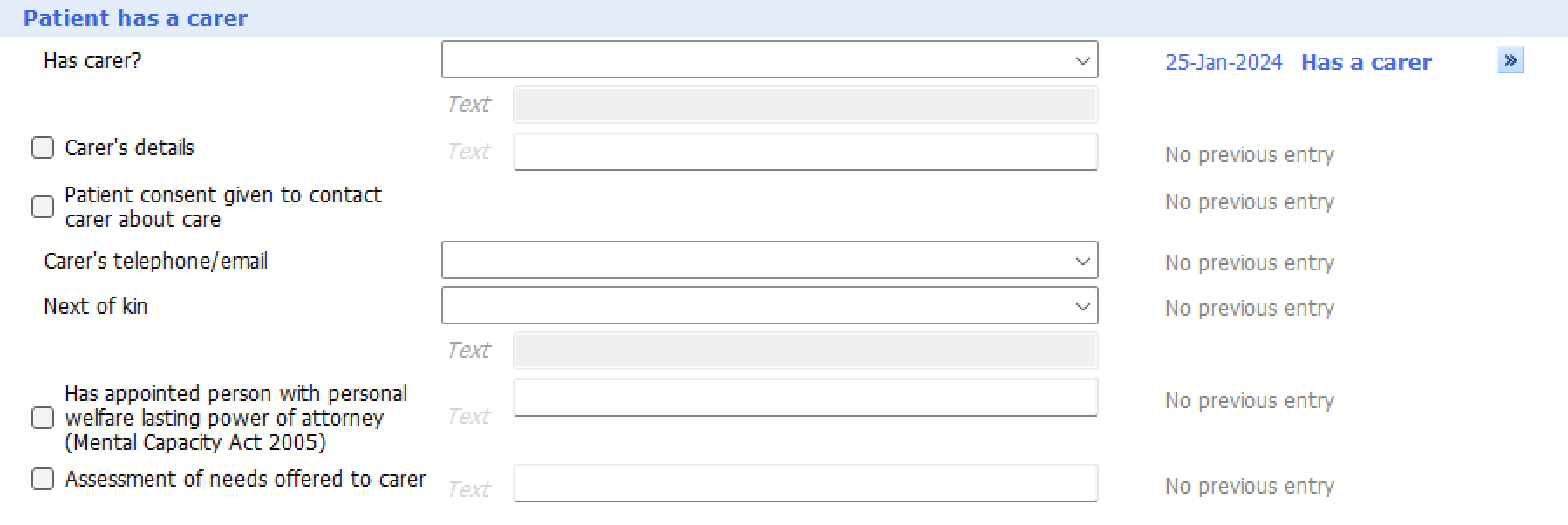
Patient has a carer
In this section, users can record whether a patient has a carer, and if so, document the carer’s details. This includes the carer's full name, contact information, and relationship to the patient. Capturing this information is particularly important when the carer plays a significant role in the patient’s daily activities, medical decisions, or ongoing care.
Consent to contact carer:
This field allows the clinician to record whether the patient consents to the healthcare team contacting the carer to discuss medical matters. This is vital for ensuring compliance with confidentiality and data-sharing regulations, as healthcare providers must have explicit permission before involving the carer in certain conversations about the patient's health.
Next of Kin or Lasting Power of Attorney:
This section also allows for the recording of a next of kin or a person who holds a Lasting Power of Attorney (LPA) for personal welfare decisions. Having this information readily available is critical in situations where a patient is unable to make decisions for themselves, as it allows the care team to quickly identify who is legally authorized to make healthcare decisions on the patient’s behalf.
Carers' needs assessment
For carers registered at the same practice as the patient, this section prompts clinicians to consider undertaking a Carer's Needs Assessment. This assessment can help identify the carer's own health and support needs, as caring for another person can often have a significant impact on the carer’s physical and mental well-being. If the carer is registered at a different practice, clinicians are encouraged to refer them to their own GP for this assessment.
Recording carer details ensures that both the patient and their support system are taken into account during care planning, enabling a more holistic and person-centered approach to managing the patient’s health.
Social Information Page
The Social Information Page is a comprehensive area where clinicians can document a wide range of social factors that may impact the patient’s health and care planning. This section is designed to be gradually filled in over time, building a full picture of the patient's social context, which is crucial for delivering personalized and holistic care.
It covers the following areas:
Sexuality and Relationships
Here, the user can record the patient’s sexual orientation, marital status, or partnership details. Understanding the patient’s personal relationships can be important in care planning, particularly when addressing sensitive issues such as sexual health or ensuring that the patient’s partner is involved in care decisions when appropriate.
Ethnic origin
This section allows clinicians to record the patient’s ethnicity using both the 2001 and 2011 census codes, as well as more generic "Ethnic Group" codes. It also includes the option to document the patient’s country of birth, which can be relevant when considering certain health risks or screening programs, such as tuberculosis screening for patients born in high-risk countries.
Religion
Clinicians can document both the patient’s religious affiliation and their level of observance. Understanding the patient’s religious beliefs can be essential when discussing care preferences, as religious practices may influence decisions around medical treatments, diet, or end-of-life care.
Mobility
This section provides space to document any mobility issues the patient experiences. Recording mobility limitations is essential for frailty and fall risk assessments, and for planning interventions that may help improve the patient’s independence and safety.
Vision
This section allows users to document any vision impairments that could affect the patient’s quality of life. Poor vision is a significant risk factor for falls and can contribute to social isolation, making it a crucial area to address during assessments.
Hearing
Clinicians can document any hearing difficulties the patient may have. Hearing impairments can lead to communication challenges, social isolation, and reduced participation in care decisions, making this an important factor to note.
Language
This section allows clinicians to document the patient’s primary language. Understanding the patient’s language needs ensures effective communication and supports the provision of care that is both culturally sensitive and linguistically appropriate. This is particularly important in consultations where language barriers could affect the quality of care.
Communication needs
In this section, clinicians can record any specific communication needs that the patient may have. This includes details such as the requirement for interpreters, the use of communication aids, or any hearing impairments that affect the patient’s ability to understand and convey information during consultations. Addressing these needs is essential for ensuring that the patient can participate fully in decision-making regarding their care.
Speech and communication
This section provides space to document any speech difficulties or other communication impairments the patient may experience. These challenges may arise from neurological conditions, injuries, or developmental factors. By recording these details, healthcare professionals can tailor their consultation style to ensure that the patient’s voice is heard and their concerns are understood effectively.
This section is where clinicians can document the patient’s driving status and any concerns about their ability to drive safely. Issues such as cognitive decline, frailty, or side effects from medication may impact a patient’s ability to drive, and recording this information helps clinicians consider potential safety risks and make appropriate recommendations, such as notifying the DVLA or referring the patient for further assessment.
Social Isolation
Clinicians can use this section to assess whether the patient is experiencing social isolation, which can significantly affect both mental and physical health. Social isolation can lead to increased risk of depression, anxiety, and other health problems. Identifying isolated patients allows clinicians to intervene early, potentially through referrals to social prescribing services or community-based support to help reconnect the patient socially.
Activities of Daily Living
This section provides space for clinicians to document the patient’s ability to perform essential daily activities, such as eating, dressing, bathing, and managing their household. Recording this information is critical for assessing the patient’s independence and identifying any need for support or care services. A thorough ADL assessment helps inform care plans that support the patient’s functional abilities and quality of life.
Nutritional Status
This section allows clinicians to assess and document the patient’s nutritional health. Poor nutrition can exacerbate existing health conditions or lead to new issues, particularly in older or frail patients. If needed, clinicians can use the MUST (Malnutrition Universal Screening Tool) score to provide a more detailed nutritional assessment and recommend interventions to improve or maintain the patient’s nutritional status. If wanting to undertake a MUST score, you may wish to use the OneCalculator template to calculate this.
Occupation / Armed Forces convenant applicable
This section is for documenting the patient’s current or past occupation, which can provide insights into their physical and mental health risks. Additionally, clinicians can note whether the Armed Forces Covenant applies to the patient, as this may entitle them to specific healthcare services or benefits. Recognizing the impact of occupation and military service on health can help guide personalized care and access to resources.
Finances
In this section, clinicians can record any financial concerns or challenges the patient faces that may impact their access to healthcare or treatments. Financial difficulties can hinder a patient’s ability to adhere to treatment plans or seek timely care. Identifying these challenges allows for appropriate referrals to social services or support programs that can help address the patient’s financial barriers to care.
Housing
Here, clinicians can document the patient’s housing situation and any factors that may impact their health, such as inadequate heating, unsafe living conditions, or overcrowding. Stable housing is a fundamental determinant of health, and understanding the patient’s living environment helps in developing a care plan that considers these social determinants. If necessary, referrals to housing support services can be made.
Alcohol screening
This section allows clinicians to record the results of alcohol misuse screening using tools such as AUDIT-C or the full AUDIT score. These tools help identify risky drinking behaviors and assess the patient’s risk of developing alcohol-related health problems. By documenting alcohol consumption patterns, clinicians can determine whether interventions, such as brief advice or referral to alcohol support services, are needed. If wanting to conduct an AUDIT-C or full AUDIT score users may wish to use the OneCalculator template
Substance misuse
This section is for documenting any history of or current substance misuse, including the use of illegal drugs or misuse of prescription medications. Understanding a patient’s substance use is critical for tailoring their care plan, particularly in managing comorbid conditions like mental health issues, or for making safer prescribing decisions. If substance misuse is identified, appropriate referrals to support services or treatment programs can be made.
Pets
In this section, clinicians can record whether the patient has pets. Pets can play a significant role in a patient’s emotional well-being, providing companionship and reducing feelings of loneliness or anxiety. However, they may also pose practical challenges, particularly if the patient’s mobility or health is declining. For example, if the patient is hospitalized or becomes less able to care for their pets, additional arrangements may need to be made, which should be considered in care planning.
Vaccinations
This section tracks the patient’s vaccination status, particularly for key vaccines like influenza, pneumococcal, and others relevant to their age or underlying conditions. Keeping these vaccinations up to date is essential for preventive care, particularly for elderly or immunocompromised patients who may be at higher risk for complications from infections. This section helps clinicians identify any gaps in the patient’s immunization history and take appropriate action.

This section has a number of elements that will show if influenza or pneumococal vaccination has been done or not, depending on the characteristics of the patient loaded
For example:
National Screening programmes
This section records the patient’s status with respect to national screening programs, such as breast, bowel, cervical, and abdominal aortic aneurysm screenings. By tracking whether these screenings are up to date, clinicians can ensure that the patient is receiving appropriate preventive care. If any screenings are overdue, the clinician can initiate referrals or schedule the necessary tests to ensure the patient’s health is monitored proactively.
This section has a number of elements that will show depending on the patient you have loaded. If highlights breast, bowel, cervical and abdominal aortic aneurysm screening status taking into account if your patient is eligible and if they have had this done or not.
e.g. if breast screening is not up to date:
Social Prescribing Page
This section is designed for documenting the activity of Social Prescribing team members. Social prescribing connects patients to community resources, such as social groups, exercise programs, or counseling services, that help address non-medical factors affecting their health. By recording social prescribing activity, this section ensures that these interventions are tracked, and their outcomes can be monitored as part of the patient’s overall care plan.
Social Prescribing
This section describes the different roles that may be seen, who may undertaken social prescribing. Because each area has chosen to approach this in different ways, you may as a PCN/Practice have all of these or none of these.
Referral and Case Finding
In this section, clinicians can document any referrals made for social prescribing or case-finding activities. Case finding involves proactively identifying patients who may benefit from additional support or interventions. Documenting these details helps track the progress and outcomes of referrals, ensuring that patients receive appropriate care and follow-up.
Details of referral
Here, clinicians can add further details about the referral, including the source of the referral (e.g., GP, self-referral) and the specific reason for the referral. This ensures that the purpose of the referral is clear to all involved in the patient’s care and provides a clear audit trail of social prescribing activities.
Appointment Narrative
This section provides a free-text box where Social Prescribing team members can document the narrative of their consultations with patients. The narrative may include the patient’s goals, issues discussed during the appointment, and any agreed-upon actions. Having this narrative documented helps build a comprehensive picture of the patient’s progress and the interventions provided.
Signposting
This section allows users to document any signposting that took place during the consultation. Signposting refers to directing the patient to relevant services or support within the community, such as exercise classes, mental health support, or financial advice. Tracking these referrals ensures that patients are connected to the resources they need and that the effectiveness of the interventions can be evaluated.
Scoring
The ONS4 Scoring Metric, as referenced in the PCN DES, is included in this section. It allows clinicians to assess patient-reported well-being across key areas such as life satisfaction, anxiety, and perceived happiness. This scoring system helps monitor the effectiveness of social prescribing interventions and can guide future support.
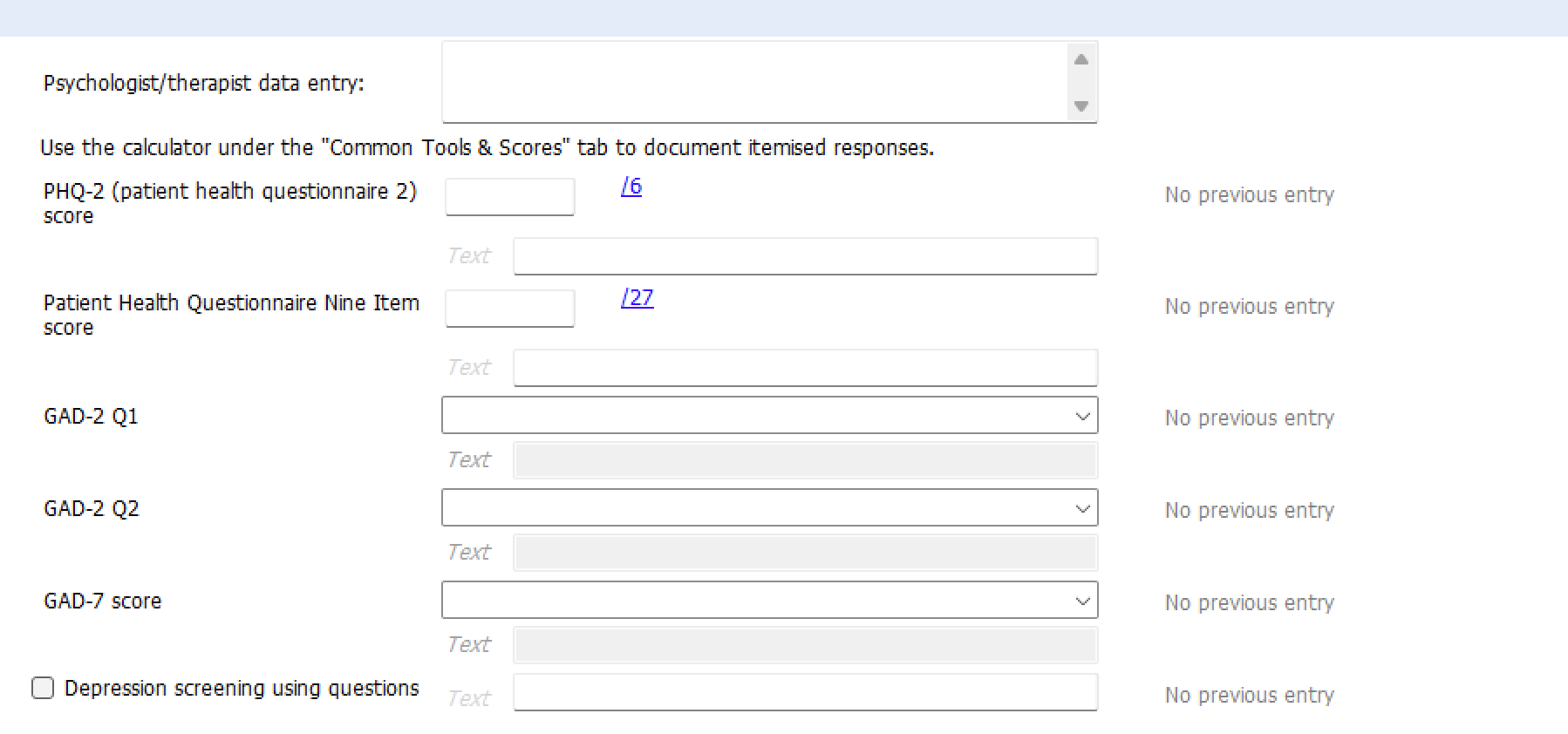
Mental Health Page
The Mental Health Page is designed to support practice-based mental health workers in recording consistent and comprehensive information about their consultations. This section ensures that mental health assessments and interventions are properly documented, helping clinicians provide continuous and coordinated care.
GAD-2 and PHQ-9:
This section includes the GAD-2 and PHQ-9 assessment tools, which are commonly used for screening anxiety and depression, respectively. The GAD-2 is a brief two-item questionnaire that helps detect generalized anxiety disorder, while the PHQ-9 is a nine-item tool that helps assess the severity of depression. Documenting the results of these assessments allows clinicians to track changes in the patient’s mental health over time and adjust treatment plans accordingly.
GAD-7:
For more detailed anxiety screening, the GAD-7 is included. This seven-item tool is widely used in primary care settings to evaluate the severity of generalized anxiety disorder. Consistently recording GAD-7 scores helps monitor the effectiveness of interventions such as medication or therapy.
Dietician Page
The Dietician Page is designed for dieticians to record patient consultations, including nutritional assessments, dietary recommendations, and follow-up plans. It includes a short-form assessment for primary care and a more comprehensive assessment typically used in secondary care.
The short form is identified as follows:
and a more comprehensive assessment in keeping with secondary care, highlighted with the following spacer:
Introduction
This section explains the purpose of the dietician assessment and guides users through the two available options: a short assessment for primary care or a more detailed assessment aligned with secondary care practices.
Encounter
Here, clinicians can record the details of the patient encounter, including the reason for the consultation, key findings, and any recommendations made. Consistently documenting these encounters allows for proper follow-up and ongoing nutritional management.
Referral source
This section allows users to document who referred the patient to the dietician, whether from within the practice, another healthcare provider, or a self-referral. Knowing the referral source helps in understanding the context of the consultation and any prior actions taken.
Discharge / Follow up
In this section, clinicians can document whether the patient has been discharged from dietetic care or if further follow-up is required. Follow-up appointments ensure that the patient’s progress is monitored and that adjustments can be made to their care plan as needed.
General History
This section includes previous blood test results and other relevant health data to aid dieticians in their assessment. Having this information readily available ensures that dietary interventions are based on a complete understanding of the patient’s health status.
Dietary History
Here, users can document detailed information about the patient’s dietary habits, intake, and nutritional requirements. This information is essential for creating a personalized diet plan that addresses the patient’s specific needs, whether for weight management, chronic disease management, or other health goals.
Physical activity level
Users may wish to use the OneCalculator template if they wish to record GPPAQ scores.
Dietetic Examination
Pharm (Pharmacist) Review Page
The Pharmacist Review Page is designed to support pharmacists in documenting structured medication reviews and other pharmacy-related activities. This section ensures that the pharmacist’s input is clearly recorded, which helps provide a holistic view of the patient’s medication management.
This section captures the type of consultation being conducted and the associated activity. Whether it’s a medication review, a reconciliation, or another pharmacy-related task, this documentation ensures clarity about the purpose and scope of the pharmacist’s involvement.
Seen by clinical pharmacist
Here, the pharmacist can document whether the consultation was carried out by a clinical pharmacist or a pharmacy technician. This distinction is important for tracking the activities of different ARRS (Additional Roles Reimbursement Scheme) team members within the Primary Care Network.
Frailty & Falls Assessment
This section serves as a quick screening tool for frailty and falls risk, providing an opportunity to capture relevant information during medication reviews. If a more in-depth assessment is needed, the pharmacist can refer to the Falls/Frailty Page for further documentation.
Proactive Care
In this section, pharmacists can document their involvement in proactive care management, which is an essential part of the PCN DES. This allows practices to track pharmacy activities in relation to proactive care and ensures that these contributions are accurately reflected in patient care.
Self management review
This section allows pharmacists to assess the patient’s ability to self-manage their medications. This is a critical part of structured medication reviews, as understanding the patient’s competence in managing their medications can prevent non-adherence and adverse outcomes.
Technical review
Here, pharmacists document a technical review of the patient’s medications, which may involve checking for drug interactions, contraindications, or appropriateness based on the patient’s clinical condition. This ensures safe and effective medication use.
Therapeutic review
In this section, pharmacists document their review of the therapeutic aspects of the patient’s medications. This may involve assessing whether the patient is on the optimal therapy, considering any potential changes, and providing recommendations to the GP or prescriber for adjustments.
Lifestyle
Pharmacists can use this section to document brief information about the patient’s lifestyle, such as smoking or alcohol consumption, which may impact their medication management. For more detailed lifestyle data, other parts of the template can be used.
Medication review
This section allows pharmacists to document the activities carried out during the structured medication review. Building up this data across the Primary Care Network will help practices demonstrate the impact of pharmacy services, particularly in improving medication safety and adherence.
Next medication review due?
In this section, clinicians can document when the next medication review is scheduled, ensuring that patients with complex medication needs are monitored regularly and any necessary changes to their regimen are made in a timely manner.
Pharm (Pharmacist) Reconcilliation Page
This page is used to document medication reconciliation, particularly when patients transition between different care settings (e.g., hospital to home). Accurate reconciliation ensures that medications are managed safely and that discrepancies between patient records are identified and addressed.
Reconcilliation
In this section, pharmacists can document the reconciliation of a patient’s medications, comparing current medications with what was prescribed during a hospital stay or other transitions. This is critical in preventing medication errors, especially for vulnerable patients.
Actions
This section allows pharmacists to document any actions taken as part of the reconciliation process, such as correcting dosages, stopping medications, or starting new therapies. By clearly recording actions taken, this ensures that all changes are communicated to the rest of the healthcare team.
DOACs Page
The DOACs Page is designed to help clinicians manage patients who are on Direct Oral Anticoagulants (DOACs), ensuring that their treatment is monitored appropriately and any potential issues are identified early. This page provides space to document important clinical details regarding the management of anticoagulation therapy.
Assessment
This section allows clinicians to record a thorough assessment of the patient’s suitability for DOAC therapy. It includes checks for any contraindications, recent test results, and patient-specific factors that could affect the choice or dosing of a DOAC.
Blood pressure
Monitoring blood pressure is crucial for patients on DOACs, as hypertension can increase the risk of bleeding. This section enables the clinician to document the patient’s blood pressure and consider whether adjustments to their anticoagulation therapy are necessary.
Diet
In this section, clinicians can record any dietary factors that may affect the patient’s DOAC therapy. While DOACs generally have fewer dietary restrictions compared to older anticoagulants like warfarin, certain foods or supplements may still have an impact, so it’s important to note any relevant dietary concerns.
Warfarin treatment
If the patient is transitioning from warfarin to a DOAC, this section allows clinicians to document details of the previous warfarin therapy. Properly managing the switch from warfarin to a DOAC is crucial to avoid complications, and this section ensures that the transition is carefully tracked.
DOAC Commencement Considerations
This section highlights any factors that need to be considered when starting a patient on a DOAC. These may include renal function, bleeding risk, or drug interactions. Ensuring that these considerations are documented helps clinicians make informed decisions about the initiation of DOAC therapy.
Already on a DOAC
If the patient is already taking a DOAC, this section provides space to record information about their current regimen. It includes options to document the specific DOAC being used, dosage, and any monitoring requirements.
If the patient is on too high or too low a dose of DOAC then warning panels are shown to highlight this
ACB Medication Page
The ACB (Anticholinergic Burden) Medication Page helps clinicians assess and manage the anticholinergic load of a patient’s medications. Anticholinergic drugs, which are often prescribed for conditions like allergies, depression, or overactive bladder, can increase the risk of cognitive decline, confusion, and falls, particularly in older patients.
Assessment:
This section allows clinicians to review the patient’s medication list and identify any drugs that contribute to the anticholinergic burden. This is particularly important for patients who are frail or at higher risk of cognitive impairment.
Management:
Here, clinicians can document any actions taken to reduce the patient’s anticholinergic burden, such as stopping or switching medications. Managing the anticholinergic load is essential for improving patient outcomes, especially in elderly populations where these medications may cause more harm than benefit.
Physiotherapist Page
The Physiotherapist Page is designed to document assessments and interventions carried out by physiotherapists. This section ensures that relevant details about physical function, mobility, and treatment plans are clearly recorded and accessible to the wider care team.
Appointment Details
In this section, physiotherapists can record the details of their consultation with the patient, including the date, time, and reason for the visit. Capturing this information helps track patient progress and ensures continuity of care.
Assessment
This section provides space to document the patient’s physical assessment, including their range of motion, muscle strength, and any pain or limitations they are experiencing. This helps inform treatment plans aimed at improving the patient’s mobility and function.
Body Maps
Physiotherapists can use this section to mark areas of the body affected by injury or pain. Visualizing the patient’s symptoms helps provide a clearer understanding of the problem and can guide the development of a targeted treatment plan.
Referrals
Here, physiotherapists can document any referrals made to other services, such as occupational therapy, pain management, or further specialist assessments. Referrals ensure that the patient receives comprehensive care that addresses all aspects of their condition.
Interventions
This section allows physiotherapists to document the interventions provided during the consultation, such as exercises, manual therapy, or mobility aids. Recording these details ensures that the patient’s treatment plan is clear and that progress can be monitored over time.
Impressions and Management
In this section, physiotherapists can summarize their clinical impressions and outline the management plan for the patient. This might include ongoing therapy, follow-up appointments, or additional interventions needed to support the patient’s recovery.
Presenting Status
This section is used to document the outcome of a physiotherapy session, specifically whether the patient attended the appointment or if it was a missed session (marked as "Did Not Attend"). Additionally, it tracks any follow-up actions that need to be taken. This section helps ensure that patient attendance is monitored and that appropriate follow-up appointments or actions are scheduled when needed.
Brief CGA Page
The Brief CGA (Comprehensive Geriatric Assessment) Page is designed to help clinicians conduct a quick yet effective assessment of older patients who may have complex health needs. It includes key elements of a CGA, allowing healthcare providers to create a snapshot of the patient’s overall health and functional status. This page supports streamlined decision-making, particularly in situations where a full CGA is not feasible.
Clinicians can document critical information such as frailty scores, cognitive function, and any urgent care needs. The Brief CGA Page ensures that important aspects of geriatric care are considered, enabling a holistic approach to the management of elderly patients.
Care Planning Page
The Care Planning Page provides a structured format for documenting personalized care plans for patients. It allows healthcare professionals to capture the patient's preferences, clinical needs, and long-term health goals. This page supports shared decision-making, where the patient and clinician work together to create a plan that addresses both immediate care needs and future care goals.
Where is Care Planning taking place?
This section is used to document the location where the care planning process is occurring. This could be in the patient’s home, in a clinical setting, or during a multidisciplinary team meeting.
Patient - About Me
In this section, the patient’s own perspective is recorded, including their personal goals, preferences, and any specific considerations they would like the healthcare team to be aware of. This helps ensure that the care plan is tailored to the patient’s individual needs.
Ethnic Origin
Here, clinicians can document the patient’s ethnic background, ensuring that cultural and personal factors are considered in the care plan. This is particularly important for understanding the patient’s preferences related to care, diet, and family involvement.
This section is where the overall care plan is developed, integrating the patient’s clinical needs, goals, and the input of the multidisciplinary team. The care plan formulation includes medical interventions, social support, and any required community services.
Patient Priorities
This section allows the patient to express their health priorities. It ensures that the care plan reflects the patient’s most pressing concerns, whether those are related to managing symptoms, maintaining independence, or achieving specific health outcomes.
Agreed Goals and Responsibilities
Here, clinicians can document the specific health goals that have been agreed upon between the patient and the care team, along with the responsibilities assigned to different healthcare providers and caregivers. This ensures that everyone involved in the patient’s care understands their role in achieving the patient’s health objectives.
Palliative Care
For patients with life-limiting conditions, this section provides space to document any discussions or decisions regarding palliative care. It includes preferences for comfort care, pain management, and the involvement of hospice services if necessary.
Resuscitation Discussion and Decisions
This section records the outcomes of discussions around resuscitation, including any advance directives or DNACPR (Do Not Attempt Cardiopulmonary Resuscitation) orders. Recording this information ensures that the patient’s wishes are respected in emergency situations.
Contingency Plans
In this section, clinicians can document contingency plans for unexpected changes in the patient’s condition. This could include action plans for worsening symptoms or guidelines for emergency contacts and interventions.
Additional Support Plans
This section provides space to document any additional support services the patient may require, such as home care, social services, or community support. These plans help ensure that the patient receives the necessary help to maintain their health and well-being outside of clinical settings.
Care Planning Codes
Care planning codes are included to enable proper coding and documentation within the clinical system. This ensures that the care plan is recorded appropriately and that relevant care activities are tracked for both clinical and reporting purposes.
Follow up
This section is used to schedule follow-up appointments or reviews of the care plan. Regular follow-ups are essential to ensure that the care plan remains relevant and responsive to the patient’s evolving health needs.